Implant-Supported Bridge Misfit: How to Improve Passive Fit in Full-Arch Cases

When a dental implant supported bridge does not seat passively, it creates a chain of clinical and mechanical problems that are difficult to resolve once the restoration is delivered. For full-arch cases in particular, achieving consistent passive fit across multiple implants is one of the most demanding challenges in implant prosthetics (and one of the most consequential when things go wrong).
This article outlines the main causes of misfit in implant-supported bridges, the clinical consequences of poor fit, and how clinicians and laboratories can structure their workflows to reduce the risk of errors from the outset.
Why misfit matters in an implant supported bridge
Passive fit refers to the absence of mechanical stress at the implant-abutment interface when a prosthesis is seated without applying any load. In single-unit restorations, minor discrepancies may be compensated for by the surrounding tissues or joint mechanics. In a full arch implant bridge, however, there is no such tolerance. Multiple implants are rigidly connected, and any gap or distortion in the framework translates directly into internal stress at each implant.
A passive fit implant prosthesis is not simply an aesthetic requirement, it is a biomechanical one. When fit is compromised, the prosthetic screws are the first components to absorb the mismatch. This leads to screw loosening, which in turn increases micromotion, affects marginal bone stability, and may eventually cause screw fracture or implant failure.
In clinical practice, fit is assessed through a range of methods: the Sheffield test, radiographic evaluation and, increasingly, digital verification steps. But prevention is always preferable to detection after the fact.

Common causes of implant framework misfit
Understanding where implant prosthesis misfit originates is essential for developing a reliable troubleshooting approach. Most problems can be traced to one or more points in the clinical-laboratory chain.
Impression and transfer accuracy
Conventional impressions using open or closed tray transfers introduce the risk of movement during tray removal, particularly when implants are divergent or when multiple implants are involved. Even small rotational errors in transfer positioning translate into geometric distortions in the master model.
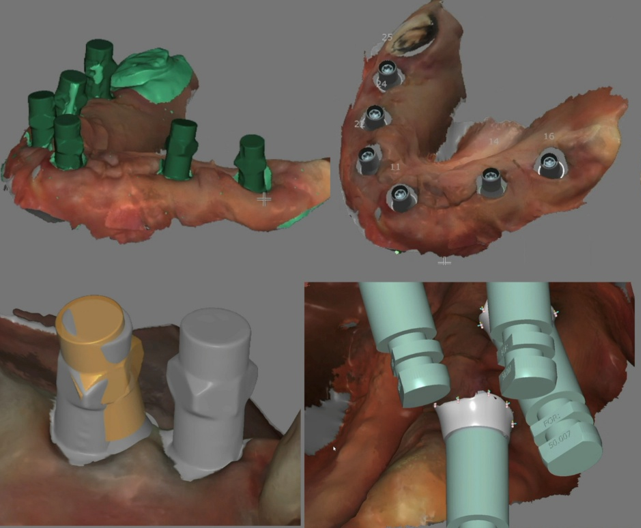
In digital workflows, the same risk exists in a different form: scanbody seating. If a scanbody is not fully seated and stable at the time of scanning, the implant position recorded in the digital model will be inaccurate. This is one of the most common and underestimated sources of dental implant misfit, particularly in full-arch cases where a small error at one implant position compounds the overall framework distortion.
Scanbody seating and dental scanbody accuracy
For digital impressions, dental scanbody accuracy depends on three variables: correct component selection, complete seating verified before scanning, and a scan strategy that captures enough reference geometry for the CAD software to identify the implant position reliably.
Selecting the wrong scanbody for a given implant system and connection type is an error that may not become visible until the framework is fabricated and returned to the clinic. By then, the cause is difficult to trace. Using verified, system-specific components and confirming seating visually or radiographically before scanning is a simple step that significantly reduces this risk.
CAD/CAM library mismatch and framework fabrication
Once the digital model is accepted, the CAD/CAM library used for design must precisely match the scanbody and the physical component that will be delivered. A mismatch between the digital library and the actual component, whether due to an outdated library, incorrect platform selection or a discrepancy in offset values, will produce a framework that cannot seat correctly regardless of how accurately the scanning was performed.
Milling tolerances, material choices and the fabrication process itself also contribute to implant framework misfit. Zirconia frameworks, for example, require careful compensation during design to account for sintering shrinkage. Any uncontrolled variable at this stage can affect the final fit.
Clinical and mechanical consequences of poor fit
The most immediate consequence of dental implant misfit in a full-arch restoration is screw loosening. When a framework does not seat passively, tightening the prosthetic screws does not resolve the underlying discrepancy, it only masks it temporarily while the mechanical stress remains. Over time, this leads to recurrent loosening, and in some cases, screw fracture.
Beyond mechanical failure, poor fit may also affect marginal bone levels, contribute to soft-tissue complications and, in the most severe cases, require a full framework remake. This outcome represents a significant cost (in time, materials and patient experience) that is largely avoidable with a structured workflow.
How clinicians and laboratories can improve passive fit
Improving passive fit dental implants requires a consistent approach across the entire workflow, from impression to delivery. The following practical measures apply regardless of whether a conventional or digital protocol is used.
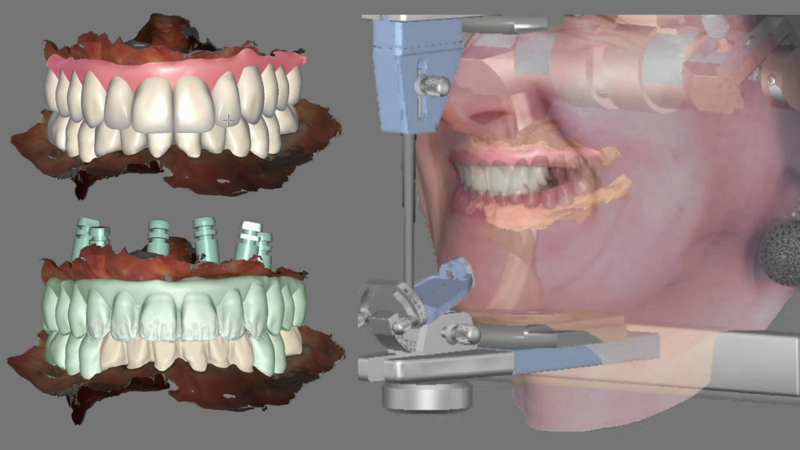
In digital workflows, a verification jig, a rigid splinted structure used to confirm that the digital model accurately represents the in-mouth implant positions, is a valuable step, particularly in complex full-arch cases or when working across large inter-implant spans. The jig is scanned or checked intraorally, and any discrepancy is corrected before the framework is fabricated. This step adds time and cost to the workflow but reduces the risk of a misfit that requires remounting or remaking.
At the laboratory level, clear communication about component specifications, scanbody selection and CAD library version is essential. Errors at this stage are preventable, but only when the clinical team and the laboratory are working from the same reference data.
How DESS® workflows support predictable full-arch restorations
One of the practical challenges in managing full arch implant restoration workflows is ensuring consistency across the components, digital libraries and verification steps used by different clinical and laboratory teams. DESS® addresses this through a structured approach to component design and digital integration.
DESS® Multi-Unit abutments are designed to work within a controlled prosthetic envelope for full-arch and multi-implant cases. Their consistent geometry and verified tolerances provide a stable reference point for both clinical placement and laboratory design.
DESS® Scan Abutments are engineered to seat fully and stably at the implant connection, reducing the risk of scanbody seating errors during intraoral or model scanning. Their geometry is validated for use with the corresponding DESS® digital libraries.
The DESS® CAD/CAM libraries are updated regularly and maintained across major CAD platforms, ensuring that the digital library used for framework design accurately reflects the physical component that will be delivered. This consistency between digital and physical reduces one of the most common sources of implant framework misfit in laboratory workflows.
Together, these elements support a workflow where errors can be identified and corrected at the digital stage, before fabrication begins, rather than at the delivery appointment when options are limited.
FAQ
What is passive fit in implant prosthetics?
Passive fit refers to a condition in which a prosthesis seats at the implant-abutment interface without generating internal stress or distortion. It means the framework contacts all implants simultaneously without any gap, rocking or load when unscrew-retained. It is considered a prerequisite for long-term mechanical stability in implant-supported restorations.
Why does an implant-supported bridge not fit passively?
The most common causes are inaccurate impression or digital transfer, scanbody seating errors, a mismatch between the CAD/CAM library and the physical component, and distortions introduced during framework fabrication. In full-arch cases, the cumulative effect of small errors at each stage is amplified across a long span.
Can scanbody errors cause misfit?
Yes. If a scanbody is not fully seated at the time of scanning, or if the wrong scanbody is used for a given implant system, the implant position recorded in the digital model will be incorrect. This error propagates through the design stage and produces a framework that cannot seat accurately regardless of subsequent fabrication quality.
Can screw loosening be related to poor fit?
Directly. When a framework does not fit passively, tightening the prosthetic screws does not eliminate the mechanical discrepancy, it compresses it temporarily. The residual stress accelerates screw fatigue, leading to recurrent loosening and, in some cases, screw fracture. Recurrent screw loosening in a full-arch case is often a sign that passive fit has not been achieved.
Clinical images courtesy of our DESS® KOL, Dt. Deni Pavlovic. These photographs are taken from his documented clinical case featuring DESS® AngleBase® solutions for upper and lower full-arch restorations. View the full clinical case here.




Dra. Patricia Isaac is a dentist and specialist in Oral Rehabilitation at DESS® and is part of our technical support department. She assists and supports our customers with technical issues about products, dental implants and prosthetic abutments, among others.
-
Thinner ANGLEBase®: Restorative Design for Narrow Implant Platforms
 July 17, 2026
July 17, 2026 -
Healing Abutment vs Cover Screw: Key Differences in Dental Implant Treatment
 July 13, 2026
July 13, 2026 -
KOL Interview: Planning, Precision & Predictability in Implant Dentistry
 June 29, 2026
June 29, 2026 -
Simplifying Restorative Workflows in Implant Dentistry with DESS® Solutions
 June 26, 2026
June 26, 2026 -
Global Partner’s Meeting 2026: Bringing the DESS® Community Together in Barcelona
 June 19, 2026
June 19, 2026